
Dentists. Dental hygienists. Dental assistants. Dental therapists. Denturists. Dental laboratory technicians. With the onset of modern technology, techniques, and materials, amended regulations, and a shift within dental education programs, it is safe to say that the roles of the dental team members have gotten a bit fuzzy. Some of what used to be taught to dentists in dental schools is no longer or is minimal at best. As a result, new graduates are looking to their team, including the lab, to play that part. In addition, some states have changed what dental laboratory technicians are legally allowed to do.
In 2020, the Florida Dental Laboratory Association pursued legislation (House Bill 713 and Senate Bill 230) that allowed the presence of a dental laboratory technician to be onsite in close proximity to the dentist while performing complex procedures, such as full-mouth reconstruction treatment plans, which generally include fabrication of a combination of dental implants and other dental devices. This change enabled a licensed dentist to request the presence of a dental laboratory technician for various treatment plan procedures and passed in the spring of 2020. Last but certainly not least, the evolution of digital has had a profound impact on doctor/laboratory communication, collaboration, and expectation.
Data provides a snapshot of how things have changed and where they are likely to go. In 2023, 31 percent of respondents to the NADL Materials and Equipment Survey indicated chairside as part of their services offered. This question was not even added until 2019.
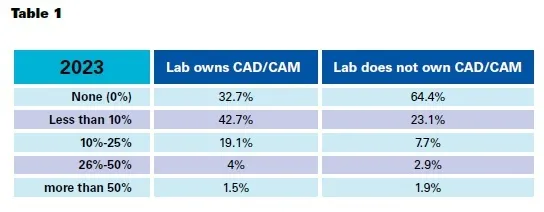
Another question asked, ‘what percentage of your business has been lost to dental clients using clinical/in-office CAD/CAM systems?’ The 2023 results displayed responses from labs that owned CAD/CAM and labs that did not (Table 1).
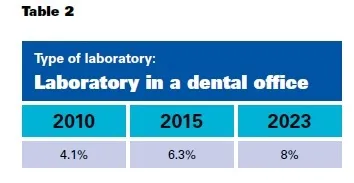
The NADL Business Survey question on the number of laboratories in a dental office also indicates an interesting increase over the years (Table 2).
The result of all these changes, whether positive or negative, really relies upon the team itself and how well each member adapts to provide high-quality results for the patient. In this dynamic, the dentist is the first and final touchpoint with the patient, and therefore, the leader of the team. Even though dental laboratories work daily with dentists and their staff, getting their candid perspectives on where the industry is going may not be in the cards.

 Meet Jackson Bean, DDS.
Meet Jackson Bean, DDS.
Talking to Dr. Bean is akin to going on a high-flying amusement park ride. The energy, excitement, and fun are palpable. What is truly unique in his case is that all that passion is directed toward dentistry. Out of dental school, he worked with Dr. Bruce B. Baird, the founder of Productive Dentist Academy (PDA). PDA was developed to train dentists how to be better businesspeople by creating efficient scheduling, production goals, and communication processes.
The evolution of digital has had a profound impact on doctor/laboratory communication, collaboration, and expectation.
In 2004, there were nine attendees at the PDA meeting, and at the most recent, there were three hundred. As a result of Dr. Bean’s intense desire to achieve advanced training in both clinical and business skills, his practice went from doing $380k a year to now doing that in a month with a team of eighteen. They have outgrown their facility and are building a teaching and surgical treatment center right across the street, featuring the latest technology in dentistry including implants by dynamic navigation. Dr. Bean recognizes that technology and education created a different playing field for the laboratory and clinician, and laboratories need to utilize those disparities to their advantage.
“Young dentists are grossly underprepared for the dental world,” said Bean. “Instead of doing 40 crowns in school they may only do a handful. Yet they don’t know what they don’t know or what they aren’t good at. Lab communication is one of those things. I have worked with many young associates and if something isn’t right, they are quick to throw the technician under the bus and want to change labs. My response, you can only run from your own problems so far, and then there won’t be any more labs to turn to. Doctors need to face the fact that they need help and mentoring. I had a great teacher and I owe my career to him along with CEREC training that provided the mirror I needed to see my mistakes. Some doctors believe they are right just because they are the dentist. This is a gross violation of human rights and I try to bring attention to it. Dental laboratory technicians want nothing more than to do the best work so dentists sing their praises. When dentists provide positive feedback to the lab, they get better results; it is basic human interaction.”
With the onset of fully digital workflows, photogrammetry, and programming software, Dr. Bean admits the necessitated computer knowledge is overwhelming for dentists. He wanted to start in-house design and searched for an in-house laboratory technician. Although the position paid well, he was unsuccessful in finding a person with analog knowledge who could fix a denture, yet also do a quick full-arch bridge in exocad. He ended up hiring a mechanical engineer graduate with zero dental experience, and in two months he had mastered the software. Although Dr. Bean regularly meets with him to teach basic dental anatomy concepts, his knowledge of the software supersedes his lack of dental; nevertheless, he can quickly provide what is needed to get the work done. This is yet another example of mixed expectations; doctors are still looking for old-school dental technicians combined with new.
Bean said, “I had to have a gold crown made the other day and it was an absolute feat. It used to be so easy to send a script. When we did all-on-fours, the lab we used had an analog technician who had done more than anyone in the country. He was very fast and very good, but when it came time to finalize, all the steps had to be taken over again. The kiss of death came at the end when the patient said, ‘I like my temp better.’ Digital is one file, and the one we print when the patient walks out is the same one as the final. The surgical center we are building has two smile suites so the patient can be a part of their own design. There is no more boxing it up and trying to communicate to the lab what the patient wants. Words get lost in written translation and now we can control that in-house. That said, there is a void of good technicians that can do a little analog stuff. They are the unicorn.”

Labs are able to experiment with technology and technique and are on the forefront of what can be done in dentistry.” – Jackson Bean, DDS
Bean works with laboratories based on predictable results, an established friendly relationship, and communication. He has at times struggled when working with new labs that had different requirements; at time patients were forced to return to the practice, giving the impression of incompetence on the part of the doctor. He emphasizes the importance of upfront communication and loves the convenience of online portals that host patient photos, instructions, and design files with immediate access. He considers the dental laboratory to be an integral member of the patient care team, and even as the responsibilities change, the role of the lab will not be diminished.
“Labs are able to experiment with technology and technique and are on the forefront of what can be done in dentistry,” he said. “We do not have to conform to old rules and methods and the laboratories that can figure things out in ways that no one sees coming will be the answer to where we flourish ahead. I just saw a photogrammetry unit on an iPhone the other day. Does it have the accuracy of the real thing? Maybe not. But where it can go is unlimited. I don’t know that big industry is going to be the answer, but I do know it won’t wipe out the labs.”
This article was originally published in the March 2024 issue of the Journal of Dental Technology.





